Anabolic steroids dependence
Anabolic steroid dependence is a complex phenomenon in which physical, psychological, and social factors are closely intertwined. Use may continue for a long time despite causing significant harm to both physical and mental health.
Updated 17 June 2026
One third of users experience dependence
It has been estimated that up to one-third of anabolic steroid users may develop dependence. This dependence is characterized by the chronic use of anabolic steroids at high doses, the prolonged use of multiple substances simultaneously, or continued use for longer than originally intended despite physical and psychosocial harms. [1, 2, 3, 16] In particular, continuing anabolic steroid use despite experiencing adverse consequences is considered the most important sign of dependence. [15, 16]
Individuals who experience dependence often have more mental health problems, difficulties with executive functioning, adverse effects, and substance use problems than users who do not develop dependence on anabolic steroids. [4, 5, 6] Dependence on anabolic steroids may also occur alongside body image disorders and exercise addiction. [15] No association between therapeutic doses of anabolic steroids and the development of dependence has been observed. [7]
It may be difficult to see how anabolic steroids could lead to dependence, in the sense that dependence or addiction is generally understood. Unlike other so-called traditional addictive substances, anabolic steroids do not cause intoxication. Anabolic steroids are mainly used in order to increase muscle mass, rather than for their effects on the central nervous system. In addition, the withdrawal symptoms that result from giving up their use are often hormonal and not the withdrawal symptoms traditionally associated with addiction. [7]
However, there is growing evidence of their effects on the central nervous system and their pleasurable effects. Anabolic steroids affect the brain’s natural opioid and dopaminergic pathways, increasing endorphin and dopamine metabolism. Just one supraphysiological injection of natural testosterone or a synthetic anabolic steroid will trigger the activation of the brain’s reward centre and increase ß-endorphin levels. This may partly explain the addictive effect of anabolic steroids, but the exact mechanism remains to be established. [8, 9, 10]
Tests on animals have shown that they will take anabolic steroids themselves when given the opportunity. Animals sometimes also take so much of the substance that it results in death. [10]
Criteria for the diagnosis of anabolic steroid dependence
There are currently no officially accepted diagnostic criteria for anabolic steroid dependence, even though there is a clear need for them. At present, anabolic steroid use is typically classified under broad and non-specific categories such as “other substance use disorder,” which makes recognition, diagnosis, and treatment development more difficult. A separate diagnostic category for anabolic steroid dependence would be important because, although it shares many characteristics with other substance use disorders, it also differs from them in several ways, particularly with regard to its hormonal effects and the context in which it is used. Such a classification could improve identification of the disorder and access to appropriate treatment in the future. [17] The research teams of Pope [4] and Kanayama [11] have created a questionnaire, which they have tested for reliability, reproducibility and validity.
Here is a set of criteria developed by these researchers. [11]
A maladaptive pattern of anabolic steroid (AAS) use, leading to clinically significant impairment or distress, as manifested by three (or more) of the following, occurring at any time in the same 12-month period:
- Tolerance, as defined by either of the following: A) A need for markedly increased amounts of the substance to achieve intoxication or desired effect; for AAS this progression to markedly larger doses may be related to dissatisfaction with the previous level of desired effect (e.g. level of muscle mass). B) Markedly diminished effect with continued use of the same amount of the substance (e.g. failure to maintain the same level of lean muscle mass on a given dose of AAS).
- Withdrawal, as manifested by either of the following: A) A characteristic withdrawal syndrome, characterized for AAS by two or more of the following features: depressed mood, prominent fatigue, insomnia or hypersomnia, decreased appetite and loss of libido. B) AAS are used to relieve or avoid withdrawal symptoms.
- The substance is often taken in larger amounts or over a longer period than was intended. For AAS, this may be manifested by repeatedly resuming courses of AAS use after a shorter ‘off’ period than the individual had originally planned, or by eliminating ‘off’ periods entirely.
- There is a persistent desire or unsuccessful efforts to cut down or control substance use. For AAS, this may be manifested by unsuccessful attempts to reduce or stop AAS use because of prominent anxiety about losing perceived muscular size.
- A great deal of time is spent in activities necessary to obtain the substance, use the substance or recover from its effects. For AAS, this may be manifested by extensive time spent participating in muscle-related activities surrounding AAS use (e.g. time spent in weight training, attending to diet and supplement use and associating with other AAS users) in addition to actual time spent obtaining and administering AAS.
- Important social, occupational, or recreational activities are given up or reduced because of substance use. For AAS, this may be manifested by giving up important outside activities because of an extreme preoccupation with maintaining a supraphysiological AAS-induced level of muscularity (e.g. the individual relinquishes outside activities for fear that these activities will cause him to miss workouts, violate dietary restrictions, or compromise his ability to use of AAS).
- The substance use is continued despite knowledge of having a persistent or recurrent physical or psychological problem that is likely to have been caused or exacerbated by the substance. Such as gynecomastia, sexual dysfunction, hypertension, dyslipidemia, cardiomyopathy, mood swings,irritability or increased aggressiveness.
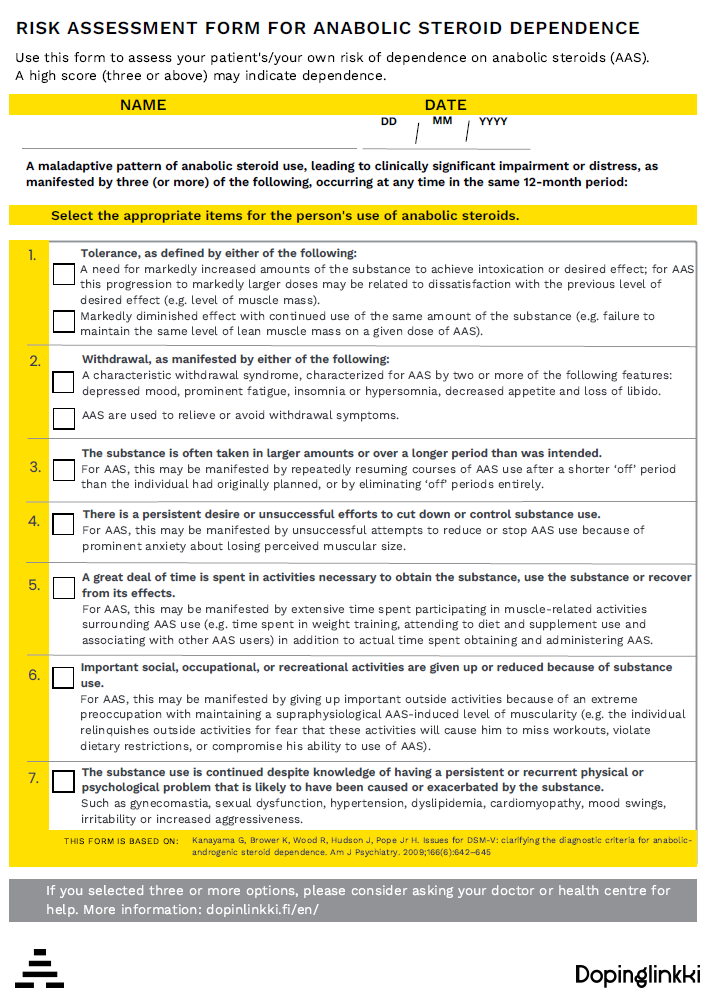
Picture: Download the PDF Risk Assessment Form for Anabolic Steroid Dependence by clicking on the picture. The form allows you to assess your own or your patient’s use of anabolic steroids and risk of dependence.’
How dependence comes about
Dependence often develops in extremely dedicated weightlifters who are highly motivated either to compete, to otherwise achieve a very muscular appearance or who want to look frightening. In addition, an environment that encourages this kind of behaviour often increases the risk of dependence. Unlike traditional addictive psychoactive substances such as cocaine and heroin, anabolic steroids do not have an immediate, strong activating effect on the pleasure centre of the brain. However, some users describe anabolic steroids as causing euphoric and antidepressive effects, sometimes quickly after injection. It could be said that anabolic steroid dependence is formed via the muscles and brain and is more complex than traditional drug addiction. [9, 12, 13]
Users have also been found to experience cravings for anabolic steroids. Craving refers to a strong desire to use these substances, for example to improve physical appearance or performance, in response to environmental cues, to maintain positive feelings, or to avoid negative ones. Craving is common among anabolic steroid users and may be an important reason for continued use, even when the formal criteria for dependence are not met. [16, 17]
Proposed mechanisms
A two-stage model has been proposed as the explanation for the development of dependence. The first stage involves using large amounts of anabolic steroids, following a strict diet and training hard to gain muscle. This stage takes up a lot of the user’s time and replaces many other aspects of their life. They may also continue the use of the substance despite social and health concerns. In the second stage, chronic high-dose usage activates the brain’s reward systems much like recreational drugs do. Psychoactive effects such as mood swings and increased aggression are features of this stage of dependence. At this stage, the criteria for dependence are met (see criteria) and the user is unable to stop using the substance despite wanting to and making the effort to do so. [12]
According to another model, dependence develops through three mechanisms. Two of these occur through the androgen receptor and the third is similar to the traditional mechanism of drug addiction. The androgen receptor produces both an anabolic and androgenic effect. In the first mechanism, the increase in muscle mass achieved through the anabolic effect can lead to the fear of losing the mass gained after quitting the substance. This involves body image problems. In the second mechanism, the androgenic effect is linked to hormonal changes and the body’s own hormonal shutdown (disorder of the hypothalamic-pituitary-gonadal axis), which occurs after quitting the substance and manifests itself as a state not dissimilar to depression and withdrawal symptoms. In the third mechanism, anabolic steroids are considered to have a direct rewarding effect on the brain via the dopamine system and to act in a similar way to the mechanisms of classical drug addiction, but at a slower rate of development. [13]
Withdrawal symptoms
Withdrawal symptoms are symptoms that occur after quitting the long-term use of an addictive substance. [14]
Quitting the use of anabolic steroids is usually followed by weeks or months of low mood, fatigue, an urge to start using anabolic steroids again, restlessness, insomnia and decreased libido. Many of these symptoms are the opposite of those experienced during anabolic steroid use, such as hypomania and increased energy, appetite and libido. [12] Psychotic symptoms are also possible during the use of anabolic steroids and may persist for weeks after quitting. In rare cases, the risk of suicide also increases after quitting. [7]
Treating dependence
There is no strong evidence for the effectiveness of the treatment of anabolic steroid dependence. The treatment is based on relatively limited scientific literature and practical experience. Treatment should initially focus on the acute withdrawal phase (hormone shutdown, drop in mood), after which it should be directed at the longer-term problems and root causes. The treatment may draw on the tools and goals used in treating other substance use disorders. These include, for example, staying off anabolic steroids and other addictive substances, treating other co-occurring mental health problems, providing social support and developing coping skills to overcome difficult situations so that relapses do not occur. [7]
Treatment for dependence may be available if the criteria for dependence are met and if other forms of addictions are present, such as alcohol or opioid addiction or amphetamine use. [7, 12]
One of the challenges of seeking treatment may be that the user does not perceive their use as harmful but, on the contrary, may see it as part of a healthy and physical lifestyle.The social environment (for example, bodybuilding and gym communities) may normalize anabolic steroid use and make it more difficult for individuals to seek treatment. Having doubts about doctors’ expertise is also a barrier to seeking treatment. [13, 17]
The treatment focuses on stopping the use of anabolic steroids and preventing the recommencement of their use. The biggest crisis in quitting is often related to the process of breaking away from the perception of one’s own body. It is no longer possible to achieve an equally strong and muscular body once the person has stopped using anabolic steroids. For some, their identity and self-esteem are very much based on their physical characteristics. Some users may even have a body dysmorphic disorder called muscle dysmorphia. [3, 12]
If the dependence involves a condition such as a body dysmorphic disorder, cognitive-behavioural therapy and SSRI antidepressants may be helpful. Especially if quitting the use of anabolic steroids is accompanied by depression. Other forms of therapy may also be appropriate, depending on the situation. For example, couple and family therapy may be helpful. [7, 12, 13]
Due to the disorder of the hypothalamic-pituitary-gonadal axis, the user’s testosterone levels can be very low after use. This can lead to depression and fatigue. Based on an assessment by an endocrinologist, treatment may be attempted, for example with human chorionic gonadotropin hormones (hCG) or selective oestrogen receptor modulators (SERM), to kick-start the user’s endocrine system and relieve symptoms. It is worth remembering, however, that it often takes weeks or months for your endocrine system to recover. In some cases, the symptoms can be very severe or it may take more than a year to see signs of recovery. [12, 13] Since there are indications of similarities between anabolic steroids and the addiction mechanisms of traditional drugs and opioids, the medicinal substances and treatments used to treat these substance disorders may also be suitable for the treatment of anabolic steroid dependence, with certain limitations. [8, 9, 12, 13]
Joni Askola, Master of Health Science, M.Sc. (Health Sci.), Dopinglinkki
[1] Kanayama G, Brower K, Wood R, Hudson J, Pope Jr H. Anabolic-androgenic steroid dependence: an emerging disorder. Addiction. 2009a;104(12):1966-78. doi: 10.1111/j.1360-0443.2009.02734.x
[2] Pope Jr H, Kanayama G, Athey A, Ryan E, Hudson J, Baggish A. The lifetime prevalence of anabolic-androgenic steroid use and dependence in Americans: Current best estimates. 2014; 23:371-377. doi: 10.1111/j.1521-0391.2013.12118.x
[3] Scarth M, Westlye L, Havnes I, Bjørnebekk A. Investigating anabolic-androgenic steroids dependence and muscle dysmorphia with network analysis among male weightlifters. BMC Psychiatry. 2023; 23:342. https://doi.org/10.1186/s12888-023-04781-1
[4] Pope H, Kean J, Nash A, Kanayama G, Samuel D, Bickel W, Hudson J. A diagnostic interview module for anabolic-androgenic steroids dependence: Preliminary evidence of reliability and validity. Exp Clin Psychopharmacol. 2010;18(3):203–2013. doi: 10.1037/a0019370
[5] Ip E, Lu D, Barnett M, Tenerowicz M, Pharm J, Perry P. Psychological and physical impact of anabolic-androgenic steroid dependence. 2012;32(10):910-919. Pharmacotherapy. doi: 10.1002/j.1875-9114.2012.01123
[6] Hauger L, Westlye L, Bjørnebekk A. Anabolic androgenic steroid dependence is associated with executive dysfunction. Drug Alcohol Depend. 2020; 208:107874. doi: 10.1016/j.drugalcdep.2020.107874
[7] Brower K. Anabolic steroid abuse and dependence in clinical practice. Phys Sportsmed. 2009;37(4):131-40. doi: 10.3810/psm.2009.12.1751
[8] Nyberg F, Hallberg M. Interactions between opioids and anabolic androgenic steroids: Implications for the development of addictive behavior. Int Rev Neurobiol. 2012; 102:189-206. doi: 10.1016/B978-0-12-386986-9.00008-9
[9] Bontempi L, Bonci A. µ-Opioid receptor-induced synaptic plasticity in dopamine neurons mediates the rewarding properties of anabolic androgenic steroids. Sci Signal. 2020;13(647): eaba1169. doi: 10.1126/scisignal.aba1169
[10] Wood R. Anabolic-androgenic steroid dependence? Insights from animal and humans. Front Neuroendocrinol. 2008;29(4):490-506. doi: 10.1016/j.yfrne.2007.12.002
[11] Kanayama G, Brower K, Wood R, Hudson J, Pope Jr H. Issues for DSM-V: clarifying the diagnostic criteria for anabolic-androgenic steroid dependence. Am J Psychiatry. 2009b;166(6):642–645. doi: 10.1176/appi.ajp.2009.08111699
[12] Brower K. Anabolic steroid abuse and dependence. Psychiatry Reports. 2002;4(5):377-387. doi: 10.1007/s11920-002-0086-6
[13] Kanayama G, Brower K, Wood R, Hudson J, Pope Jr H. Treatment of anabolic-androgenic steroids dependence: Emerging evidence and its implications. Drug Alcohol Depend. 2010;109(1-3):6-13. doi: 10.1016/j.drugalcdep.2010.01.011
[14] Terveyskirjasto. Vieroitusoire. Lääketieteen sanasto. 2016. Duodecim oy.
[15] Scarth M, Westlye L, Havnes I, Bjørnebekk A. Investigating anabolic-androgenic steroid dependence and muscle dysmorphia with network analysis among male weightlifters. BMC Psychiatry. 2023;23–342
[16] Carter B, Boardley I. Development and validation of dependence and craving measures specific to athletes who use anabolic-androgenic steroids. Front Psychol. 2024:15:1347211. DOI: 10.3389/fpsyg.2024.1347211
[17] Scarth M, Havnes I, Bjørnebekk A. Anabolic-androgenic steroid use disorder: case for recognition as substance use disorder with specific diagnostic criteria. Br J Psychiatry. 2025:1-5. DOI: 10.1192/bjp.2025.73
Like, share